Can Colored Contact Lenses Diolade With Light
Colored contact lenses are used for more than what typically comes to mind—special movie effects and eye color enhancement. They can also be used therapeutically to alter vision or prosthetically to mask ocular disfigurements. Sometimes, a patient has a multitude of ocular issues requiring both therapeutic and prosthetic care. Myriad ocular conditions stand to benefit from colored contact lenses. This article helps eye care practitioners select and manage the proper contact lens for various clinical uses.
 |
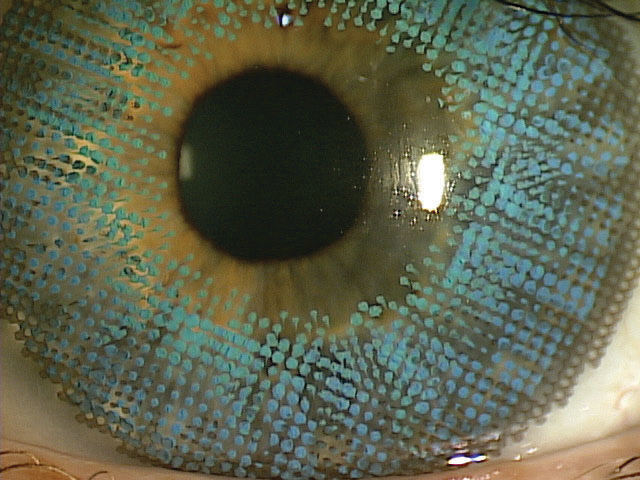
| Blunt ocular injury left this eye aphakic with a ruptured iris, irregular pupil and scarred ocular surface. Placement of a prosthetic contact lens by Crystal Reflections restored the patient's cosmetic appearance and gave her the confidence to continue her social interactions. Photos by Christine Sindt, OD. Click image to enlarge. |
Know Your Options
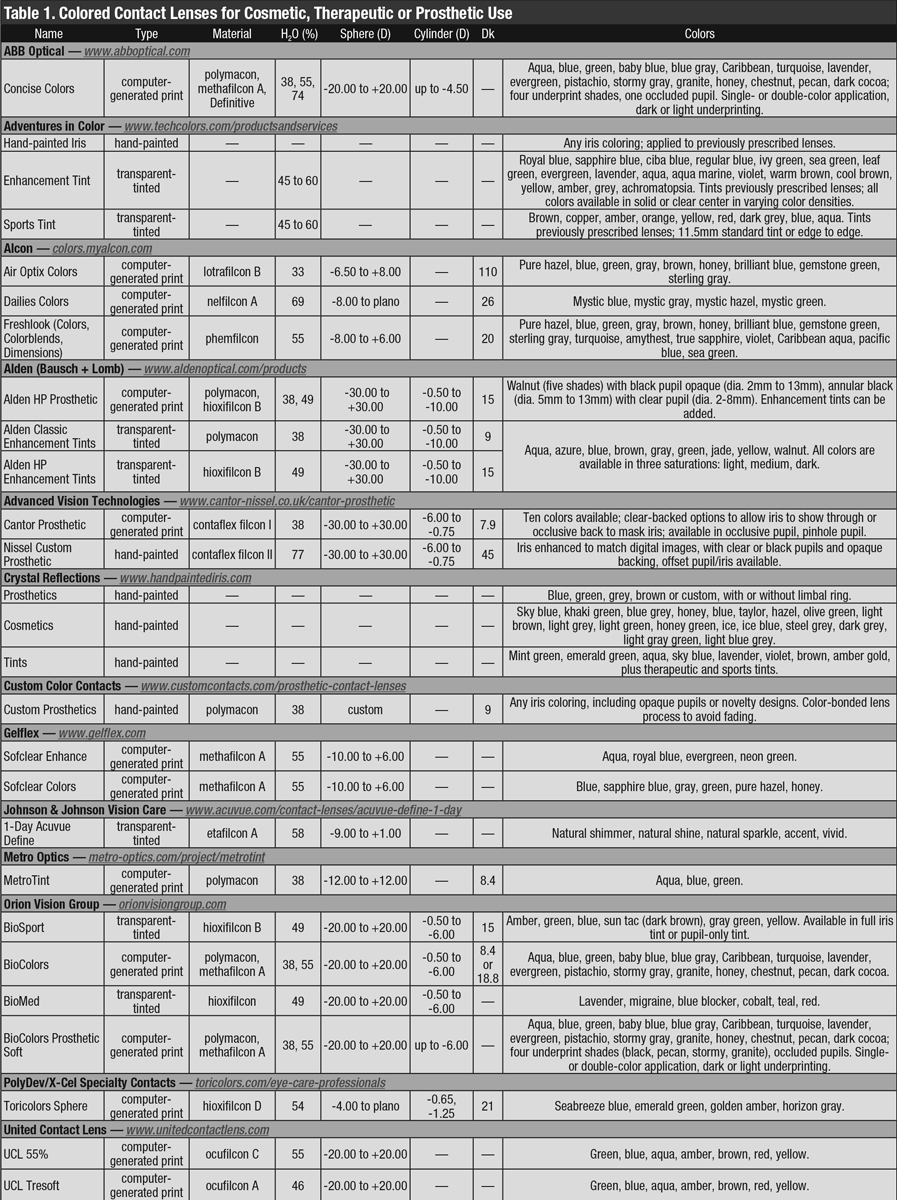
First made commercially and widely available in the 1980s, colored contact lenses have evolved to satisfy the fashion-forward patient's desire for cosmetic change and improvement. Currently, these lenses are made in both HEMA and silicone hydrogel (SiHy) materials. Three main types of colored contact lenses can be used cosmetically, therapeutically or prosthetically for different ocular conditions (Table 1):
Transparent-tinted contact lenses. These lenses are fit to alter a patient's perception, especially in the case of sports (e.g., green tints can make a tennis ball appear darker, yellow tints can enhance the incoming image of a baseball, blue or violet tints can minimize glare for snowboarders), photophobia and color blindness. They can decrease stray light affecting the cornea, iris, lens and retina, effectively limiting ocular glare.1
This option has a uniform iris color with varying pupil sizes. The transparent tint overlaps the natural iris background, causing the iris to change in color and offering a more natural look. The iris background can be seen through contact lenses with lighter tints. Darker tints, such as a dark brown, may mask some corneal or iris irregularities, though not as effectively as computer-generated opaque and hand-painted custom contact lenses.
Full iris occlusion is not easily obtainable and, for light-colored irides that require a prosthetic lens, it may be hard to match the color of the eye with the lens. It is also difficult to obtain complete pupil occlusion if the black pigment is not dense enough. Again, computer-generated or hand-painted contact lenses may be more effective.
Clear, translucent-tinted and black pupils are available in a variety of pupil sizes, but there is a low degree of customization; iris and corneal details—such as pupillary ruffs and corneal arcus—are not available.
These lenses are easily reproducible and, thus, comparatively inexpensive relative to custom lenses. They are made of HEMA material, as the low water content of SiHy lenses does not allow them to tint well.2 Due to limited color and pupil options, less chair time is required compared with custom, hand-painted lenses. While diagnostic sets are available from certain manufacturers, others can tint lenses already prescribed to the patient or provide consulting assistance for empirical fits.
Computer-generated opaque contact lenses. While transparent-tinted lenses have a uniform iris color, these opaque contact lenses have a variety of computer-generated patterns, colors and pupil sizes layered onto the lens to increase the availability of options that range from a natural, subtle look to a bolder statement. Some manufacturers offer the option to add a black, white or clear iris backing. Black or white options offer full iris occlusion to mask most iris irregularities, while clear backings allow some of the natural iris details to be seen through the lens. The color of the backing can influence the perceived iris detail and color on the front of the lens, which needs to be taken into consideration when color-matching. For some patients with darker irides, a black color can provide complete iris occlusion and be a suitable cosmetic match to their eye. Some manufacturers offer subtle enhancement options regarding iris details, pupillary frills and limbal rings.
| |
| This 39-year-old female with multiple sclerosis and optic neuritis has severe photophobia and must use sunglasses, even while indoors, to deal with the pain. She is now wearing Alden HP 49 lenses with full tint walnut brown #3 and, as she puts it, "I've got my life back." She only wears sunglasses outdoors now and likes her new brown eyes. Photo by Bruce Baldwin, OD. Click image to enlarge. |
Since the lenses are computer-generated, their limited templates and color options make them more reproducible, with good consistency. These lenses do not fade. They are also easier to fit and require less chair time at a lower cost compared with painted lenses. Some can be replaced frequently, which improves comfort and decreases complications common with annual replacement lenses.
They are primarily available in HEMA materials, though one disposable, high Dk SiHy lens, Air Optix Colors (Alcon), is available and can be especially important for oxygen-compromised corneas. Diagnostic lenses are available from certain manufacturers, and other companies can provide consulting assistance for empirical contact lens fittings.
Hand-painted custom contact lenses. These lenses have the highest level of customization and can be produced on HEMA soft lenses or painted on scleral lenses in any color with any iris diameter and pupil size. An ocularist can add details, such as iris nevi and blood vessels, to match the eye. These lenses can conceal severe ocular disfigurements. For example, the position of the iris can be painted offset from the underlying iris in strabismic eyes to make a patient's eyes appear aligned.
The iris is painted on a clear, white or black backing. Depending on the look the patient is going for, black can make the surface color look darker and reduce glare and photophobia. Patients with light iris colors get the best of both worlds with these lenses, as they're dense enough to provide contrast and not too dark for a good cosmetic match.
To order these lenses, a photograph of the fellow eye is sent to a contact lens lab. Once the patient approves the lab's attempt at color-matching, the custom lens is made. Expect to wait several weeks to months to get the final lens. It may be worth consulting with your contact lens manufacturer, especially as these are the most expensive option, because generally there are limited warranties, and often once the lens is ordered, it cannot be changed or returned. Follow the manufacturer's cleaning recommendations to minimize fading, especially as the low Dk lenses are replaced annually.
 |
| Click table to enlarge. |
Manage Ocular Conditions
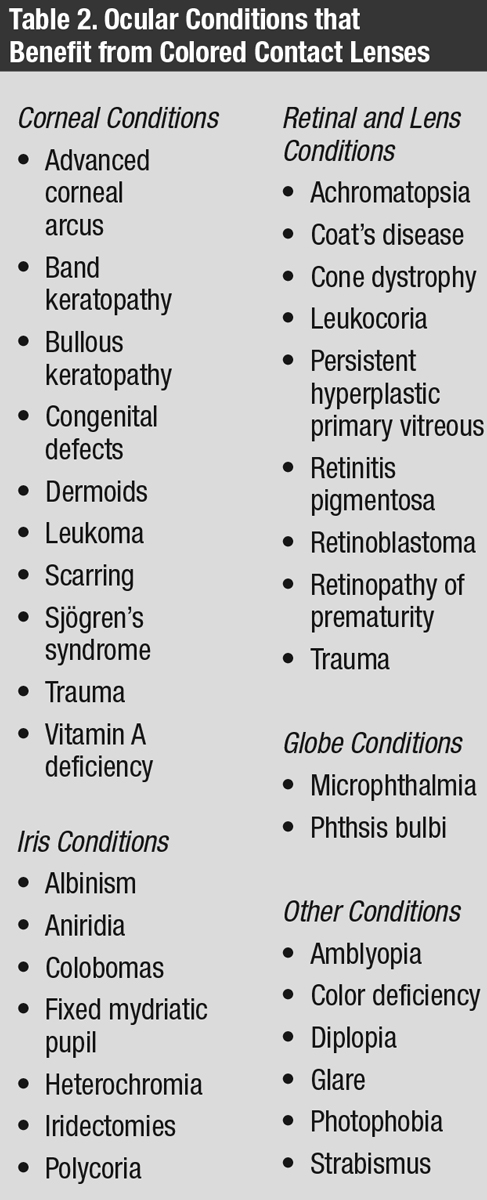
Colored contact lenses can benefit a handful of different ocular conditions (Table 2). These lenses can be more cosmetically appealing than other options, such as wearing a patch, and increase patient compliance.
Corneal conditions. Any patient with corneal opacification can benefit from a prosthetic contact lens. The size and location of the corneal scar and the color of the iris will dictate the type of lens needed. For patients who can still see, choose a clear pupil. Consider a SiHy material if the cornea is compromised, as it can benefit from the higher Dk. SiHy lenses with a high Dk can also be beneficial when piggybacked below a gas permeable contact lens on a keratoconus patient who is experiencing excessive glare. Note that paint-on, custom painted lenses may also decrease oxygen permeability through low Dk HEMA lenses.
Iris conditions. When working with iris abnormalities, such as heterochromia, tinted or opaque contact lenses can cosmetically alter the differing iris colors of two eyes to make them look more similar. Enhancing tints blend with the underlying iris for a more natural look.
Iris defects often cause symptoms of glare and photophobia. In conditions such as aniridia, polycoria, colobomas and iridectomies, a colored lens with a clear pupil will reduce glare, provide normal light perception and cosmetically improve the appearance of iris defects, especially in the case of iris colobomas. Recommend a clear pupil and matching opaque iris for patients who have fixed mydriatic pupils from trauma or disease to reduce the glare. Colored contact lenses should be a viable option when attempting to reduce glare, as solutions such as corneal tattooing are more invasive and permanent.3
Seven percent of patients with iridectomies have visual symptoms of shadows, ghost images, crescents or lines, which are more prominent in cases of exposed iridectomies.4 The colored annular iris of prosthetic contact lenses benefits these patients.
For albino patients whose lack of pigmentation causes extreme photosensitivity, darker colored contact lenses can act as filters. Compared with sunglasses, contact lenses provide complete pupillary coverage, limit peripheral glare and eliminate rear surface reflection. The diameter of the colored iris should be 2mm to 3mm larger than the patient's pupil in dim illumination. Because visual acuities may be significantly reduced in low light illumination, a moderately tinted contact lens should be prescribed. Sunglasses and hats should still be worn.
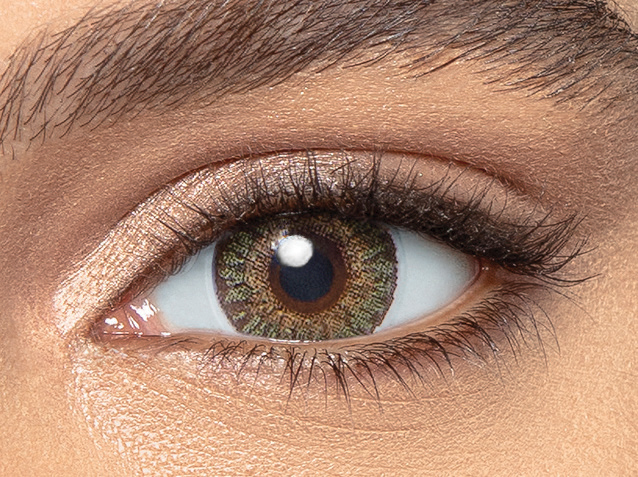 |
| Alcon Dailies Colors bring eye-changing capability to the daily disposable modality. Pictured is Mystic Green, one of four options in the new product line. Photo by Alcon. Click image to enlarge. |
Retinal and lens conditions. The pupil may appear white due to certain lens conditions, such as leukocoria, or retinal issues, such as retinopathy of prematurity, retinoblastoma, persistent hyperplastic primary vitreous, Coats' disease or trauma. For non-seeing eyes, a black pupil with a matching opaque iris can improve a patient's self-esteem.
Uniform, dark brown contact lenses can be fit on patients with Bothnia dystrophy, a variant of retinitis pigmentosa with a prolonged dark adaptation. These lenses, worn only during the day, maximize visual potential by decreasing glare and extreme light sensitivity to improve orientation and mobility. The darkness of the tint is adjustable depending on the light intensity of different seasons.5
Cone dystrophies and achromatopsia can also cause severe photophobia. Similar to congenital color vision deficiency, these conditions reduce color vision and visual acuity but can also be accompanied by central scotomas and nystagmus.6 Tinted contact lenses decrease photosensitivity, improve visual acuity, decrease the size of central scotomas, enlarge the peripheral visual field and enhance the visibility of long-wavelength stimuli in bright illumination.7 Red lenses, especially in patients with achromatopsia, decrease the amount of short-wavelength light, reducing rod photoreceptor activity.8,9
The density and the tint color prescribed depends on the severity of the disease and the type of cone dysfunction. Red-brown tints may be more suitable for patients with residual cone function, and magenta may be favorable in cases of blue cone monochromatism.7,10 Some recommend amber, gray or a combination of colors with a transmittance value of 14% to 30%.8,10-12 To minimize debilitating photophobia, one study fit patients with cone disorders with red-tinted contact lenses, which immediately decreased their photophobia and improved their residual vision, allowing eight of the 23 participants to become eligible to drive.8
Globe conditions. For patients with smaller ocular globes, such as in cases of phthisis bulbi or microphthalmia, painted scleral shells can fill in for the lost orbital volume ö and realign the lid to a more normal position. The smaller eye can also appear bigger with a limbal ring and a clear contact lens fit on the normal eye. For extreme disfigurements, a prosthetic scleral shell may be an alternative to enucleation or evisceration.13
Other conditions. Tinted lenses cannot cure congenital color deficiencies, but they may help improve color discrimination by modifying the light spectrum and altering brightness and hue saturation.14 For red-green color deficiencies, a red-tinted lens fit on the non-dominant eye can aid in color contrast.
An all-black contact lens (black pupil and iris) can remove all extraneous visual stimulation to eliminate diplopia. An appropriate front iris color can be printed on top to match the other eye.
 |
| Natural Sparkle 1-Day Acuvue Define lenses are designed to brighten light eyes. Photo by Mile Brujic, OD. Click image to enlarge. |
Changing the size of the black pupil and the pattern of the iris print on colored lenses allows customization of visual penalization and leaves the peripheral fusion intact during amblyopia treatment.15,16 The larger the opaque pupil, the greater the visual penalization. A color-matching lens with a clear pupil can be fit on the other eye to improve cosmesis.
A hand-painted scleral lens can be fit on a strabismic, non-seeing eye with the iris painted off-center to match the visual alignment of the other eye. The lens should be fit large and truncated for good stability and opaque to mask the underlying, off-centered iris. In the case of a prosthetic soft lens, use prism ballast to prevent rotation. The good eye should help you determine where the new pupil should be. For severe ocular disfigurements, gather information from the good eye, including corneal topography, pupil size (in low, normal and bright conditions), iris diameter and matching iris color.
Set Expectations
As eye care professionals, we emphasize the treatment of underlying ocular pathology and the management of ocular health, but we must not neglect the emotional aspect that comes with patients who receive these services.
While colored contact lenses should be fit to maximize vision, prepare patients that these lenses can decrease and/or change their visual perception. Determine the functional needs and priorities of those who opt for therapeutic or prosthetic lenses. While this modality aims to marry cosmesis and vision, have patients choose which is more important to them. For non-seeing eyes, the priority is cosmesis, but for sighted eyes the patient may have to compromise, and their decision will dictate their options and outcomes.
For patients whose primary goal is cosmesis, be mindful to set realistic expectations. With current technology, colored contact lenses can look similar enough to the unaffected eye from a distance but will not be an exact match up close. While the iris and pupil are about 3mm to 4mm behind the cornea in a normal eye, the artificial iris and pupil are at the surface of the colored contact lens. Additionally, dot matrix color designs of computer-generated, printed contact lenses may appear artificial.
The fitting process, especially with custom, painted contact lenses, is expensive, time-consuming and complex, often requiring multiple visits. Because these lenses are generally low Dk and replaced annually, more frequent follow-up visits are necessary. The difficulty in fitting cosmetic lenses does not usually lie with the lens itself but with managing patient expectations.
 |
| Brilliant Blue Air Optix Colors are designed to blend with and enhance natural eye color. Photo by Mile Brujic, OD. Click image to enlarge. |
Be Aware of Complications
Maintaining ocular health is always the most important aspect of fitting contact lenses. The eye must be able to support a lens with good fit and comfort. Unfortunately, sometimes contraindications occur, including blebs, sutures, dry eye and ocular allergies. Consider a SiHy contact lens to decrease conjunctival hyperemia and reduce the risk of corneal neovascularization, especially if there is an associated risk of corneal allograft rejection, corneal edema or bullae, all of which may lead to corneal decompensation.17,18
Trial a clear contact lens to ensure the eye can sustain contact lenses before ordering a colored one. A larger diameter will provide better centration and less lens movement for better cosmesis, though the lens cannot be too tight to limit tear exchange.
For those who use glaucoma medications, removing contact lenses to instill drops during the day may not be the most convenient option. Prescribing less frequent drug dosing will not only improve patient compliance but also make it easier for those who wear contact lenses.
For amblyopia or monocular patients, prescribe polycarbonate spectacle lenses over contact lenses to protect the good eye. If the prosthetic eye is smaller in appearance, consider magnification with a plus lens in the spectacles to enlarge the eye or lid aperture. An antireflective coating or a light tint may also help camouflage the discrepancies between the eyes behind the glasses.
Before working with prosthetic lenses, it's important to understand that the rate of lens-related complications is higher. A pair of studies found the rate to be 40% compared with 20% in conventional soft lenses.19,20 Solid pupil-colored contact lenses had a significantly higher complication rate than lenses with clear pupils, with higher incidences of giant papillary conjunctivitis, superficial punctate keratitis and corneal erosion.19 Prosthetic contact lenses can also worsen meibomian gland dysfunction, induce allergic reactions or toxic keratopathy and cause trauma to the corneal and conjunctival epithelium.21,22
 |
| Click table to enlarge. |
The risk of infection is always higher for those who wear contact lenses. Take extra caution when considering the risk-benefit ratio of colored lenses for patients who can see and prioritize cosmesis. A custom prosthetic lens may be cosmetically appealing, while a more disposable, computer-generated, printed SiHy contact lens may be healthier.
The colored annular iris of colored contact lenses can affect vision in seeing eyes. Tinted lenses reduce the optical quality in higher-order aberrations, which may decrease contrast sensitivity and night vision.23-25 One study found that hand-painted, opaque, annular soft contact lenses decreased sensitivity over the central 120 degrees in subjects with normal vision.26 Opaque- or semi-opaque-tinted contact lenses reduce the amount of light reaching the retina, resulting in decreased vision in mesopic or scotopic conditions.
Annular colored lenses can also cause visual field constriction, with one study finding that such a lens with a 5mm pupillary zone decreased visual fields by 21% to 47%.27 Another observed a 10-degree scotoma nasally and temporally beyond the central 30 to 50 degrees from fixation, which corresponded with the opaque iris surrounding the central 5mm clear optical zone.28 As the diameter of the annular pupil decreases, photophobia and glare improve at the expense of the visual field. It's important to strike a balance between visual comfort and field-of-view. For patients who are primarily indoors, match the final pupil diameter to the normal pupil in dim illumination. For those who spend more time outdoors, match the final pupil diameter to the normal pupil in light illumination.
Colored contact lenses are underused but versatile options for a population of patients who stands to benefit from them. Therapeutic colored contact lenses can help those who have working vision see the world more comfortably. For those who require extra aid, prosthetic colored contact lenses can improve their physical appearances and self-confidence. Colored lenses not only broaden the optometrist's scope of practice but also improve the quality of many lives.
Dr. Yeung is a Diplomate of the Cornea and Contact Lens Section of the American Academy of Optometry and a senior optometrist at the University of California, Los Angeles (UCLA) Arthur Ashe Student Health and Wellness Center.
Ms. Wong graduated from UCLA with a degree in psychobiology. She is an optometry patient care representative at the UCLA Arthur Ashe Student Health and Wellness Center.
Can Colored Contact Lenses Diolade With Light
Source: https://www.reviewofcontactlenses.com/article/colored-contacts-more-than-a-pretty-eye